Clinic Station Flow
Overview
In order to maximize every inch of space, maintain high quality surgery and achieve a positive, enjoyable working environment, an efficient workflow is critical. All of our cats are within grasp and sight throughout all stages of their visit, particularly during induction and recovery. Keeping every station in the same room allows immediate and smooth orchestration from one station to the next. Our volunteers work as a team; constantly in contact with the cats, the doctors and the volunteers, ensuring that our cats receive high quality spay/neuter services.
We truly are a small organization doing BIG work.




Check-In
CLINIC POLICIES
Our policies differ from many programs. We minimize as many obstacles as possible, to increase access to spay/neuter. In our experience, if the process is too difficult, too time-consuming, too frustrating or too confusing, people give up and the cats lose.
Read More
Clinic Policies
Why Did We Establish These Clinic Policies?
STEP 1: BEFORE CATS ENTER THE CLINIC
From 7:00 AM until 8:30, cats come through the door. Caretakers must complete many Check-in criteria before the cats leave the car.
Read More
Before Entering Clinic
Check-in Poster
Why We Do it This Way
1. Whose signature do we require on a Surgical Release Form?
The Surgical Release Form has two main purposes: To protect an owned cat from being brought to the clinic without the owner’s knowledge; and to protect our organization from liability. Trappers and neighbors do not always seek out whether cats have owners or whether owners permit their cats to be altered. We adamantly discourage this practice. If an owner were to object and complain that we altered or ear tipped their cat, then we have a signed waiver of who acted as the cat’s agent. That individual would be accountable for the consequences.
We request a Surgical Release Form from the person transporting the cats, from the person who made the reservation and from the person who is primary caretaker. Ideally, we want a Surgical Release Form from the person who would make the decision to adopt out or euthanize the cat, that is, the person who is most intimately connected and responsible for the cat. If not all waivers are available on the morning of surgery, then we require at least one Surgical Release Form be completed at each clinic from someone who has the legal responsibility for making decisions regarding the cats. No cat is accepted into the clinic without a signed Surgical Release Form from the transporter, the person making reservations or the caretaker.
2. Why do we require one Medical Record per cat?
There are two basic systems for tracking procedures through a high volume spay/neuter clinic. Some clinics compile a list at each station that documents what each cat receives as it goes through. For example, a list at the FeLV testing station would document IDs of which cats were tested and their results. We prefer a system of individual medical records, so that each cat has a comprehensive list of what was observed and administered.
If there are any complications during the clinic, all information is with the cat, because the Medical Record does not leave the cat. We can simply look at that cat’s record and find what information we need right away. We file the Medical Records by clinic date, so if there is a question any time after a clinic, it is easy to retrieve the information.
STEP 2: CATS CHECK-IN
Properly identifying cats begins here. Our system maintains identification, gives us an efficient visual marker for monitoring cats pre and post op and generates donations.
Read More
Why We Do it This Way
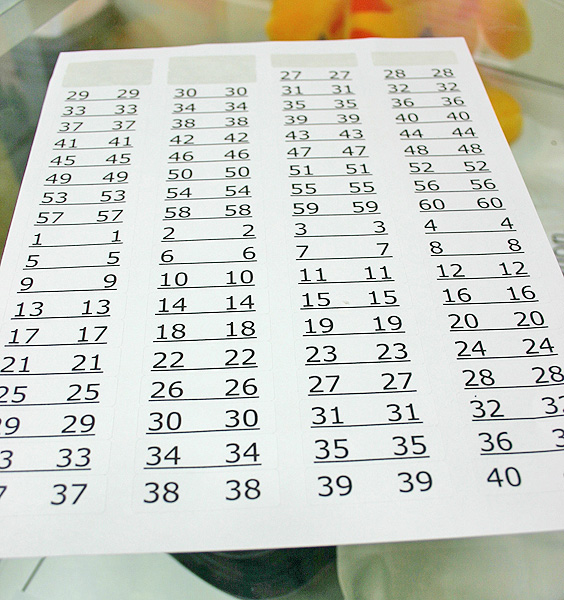
1. Why do we use preprinted labels that are difficult to remove instead of handwritten numbers on masking tape?
We began using preprinted stickers for several reasons: to save time and to eliminate mistakes reading ID numbers. Poorly written handwritten ID numbers can be misread causing mix-ups of cats and carriers during the clinic.
The labels that we use are very sticky, so that they adhere well. Some brands of labels fall off easily leaving carriers and traps unidentified. At first, some caretakers complained that the stickers were hard to remove, but we reminded them of the importance of proper ID.
Another benefit to preprinted labels is to prevent accidentally duplicating or skipping ID numbers during a cat. This occurred occasionally when we used masking tape and handwritten numbers. Duplication of a number could lead to cats being switched and getting returned to the wrong caretaker. Omission of a number leads to serious distraction and disruption of clinic flow while we figure out whether a cat has accidentally been skipped or if the number was never assigned. Preprinting labels avoids these problems.
2. Why do we put masking tape on the trap when the cat is being transferred to a carrier after surgery?
There are millions of outdoor cats bringing homeless kittens into this world each year. In our experience, many of these unaltered cats are be social, loving companions to people who have not pursued spay/neuter. Others formerly had homes with people who never altered them and for myriad reasons, the cats now live on their own and are known as “strays”. Some cats have never known a life with people while others have reverted to unsocial behavior.
When a cat is afraid of people, no one can truly differentiate whether it was born without human exposure or whether it formerly had human exposure and became unsocialized. The distinction does not really matter. The term “feral” describes a particular behavior, that of a cat that is not used to people or is not trusting of people in its current set of circumstances.
In private veterinary practice, feline patients can be affectionate and loving to their human family, yet require general anesthesia before a veterinarian can examine it. This behavior is called “fractious”, because the cats exhibit social behavior with people at home. But if a fractious cat were found and taken to a shelter, its behavior could earn it the label “feral”. There would be no way to know that in the right circumstances that the cat is socialized.
Furthermore, many people know “feral” cats that developed social behavior after extended and consistent positive human interactions. Such progression to social behavior or taming is actually predictable, especially considering that true wildlife - squirrels, raccoons, deer, etc - become conditioned to hand-feeding or touching after extended periods of positive human interaction. Domestic, free-roaming cats are no exception.
Simply stated, “feral” denotes a behavior, and behaviors can be modified, in many cases. Regardless of whether a cat loves people or fears them, any outdoor, unaltered cat is reproducing and contributing to the homeless cat problem. We find that “free-roaming” the best descriptor for these cats. Distinguishing feral-behaving from free-roaming is unnecessary.
Tame cats can usually be examined rather easily. Cats with feral behavior are a bit trickier. If they are in traps, we feel the cat for testicles under the tail through the bottom of the trap. We may or may not need to use the trap divider for this. Big-cheeked tom cats need no exam. They are pretty obviously male. Tortoiseshell and calico are always female, for practical purposes. Occasionally, we will put cats in the capture net and examine the genitalia by palpation to see if we feel testicles. Although lack of testicles is not a guarantee of a female, it is almost a guarantee that the cat is not a tom cat.
STEP 3: ARRANGING CATS FOR EFFICIENT FLOW
Our stainless steel tables provide plenty of room for stacking carriers and traps. Grouping cats by gender and priority improves efficiency and greatly increases clinic flow.
Read More
Arranging Cats for Efficient Flow
Flow Floorplan
Why We Do it This Way
1. Why do we use stainless steel tables?
The primary benefit of stainless steel tables is that they are easy to disinfect. They are lightweight, restaurant tables that have adjustable lower shelves to meet the needs of our space. The back edge of the top level prevents anything from spilling off the back of the table. We purchased them from a restaurant supply company, and they were much less expensive than stainless steel tables sold for hospital use. Although we do not use them, casters can be purchased so that the tables can be rolled around.
2. What distinguishes a “free-roaming” cat from a “feral-behaving” cat?
There are two basic systems for tracking procedures through a high volume spay/neuter clinic. Some clinics compile a list at each station that documents what each cat receives as it goes through. For example, a list at the FeLV testing station would document IDs of which cats were tested and their results. We prefer a system of individual medical records, so that each cat has a comprehensive list of what was observed and administered.
If there are any complications during the clinic, all information is with the cat, because the Medical Record does not leave the cat. We can simply look at that cat’s record and find what information we need right away. We file the Medical Records by clinic date, so if there is a question any time after a clinic, it is easy to retrieve the information.
3. Why do we need to know gender?
There are two basic systems for tracking procedures through a high volume spay/neuter clinic. Some clinics compile a list at each station that documents what each cat receives as it goes through. For example, a list at the FeLV testing station would document IDs of which cats were tested and their results. We prefer a system of individual medical records, so that each cat has a comprehensive list of what was observed and administered.
If there are any complications during the clinic, all information is with the cat, because the Medical Record does not leave the cat. We can simply look at that cat’s record and find what information we need right away. We file the Medical Records by clinic date, so if there is a question any time after a clinic, it is easy to retrieve the information.
Cost Saving Tips
1. Why use stainless steel tables instead of hospital tables?
We use stainless steel restaurant tables to hold all the cats. Easily disinfected, they last a lifetime. With a top and bottom level, many cats can be stacked in a small footprint of space. Tables are produced in a variety of widths and lengths. We purchased ours new, because we needed a specific configuration and sizes. Used tables are also available at reduced prices from used restaurant supply stores.
Anesthesia



OUR ANESTHETIC COCKTAIL
Learn how small differences in our anesthetic protocol reduce risk and unexpected mortality to half the national average.
Read More
Why We Do it This Way
1. Why do we use TKX instead of other newer anesthetics?
We want an anesthetic protocol that is predictable and proven safe in tens of thousands of cats in varying stages of health. We need an injection that is given intramuscularly, is widely available and is economical. Because we send home cats on the same day as surgery, we need the anesthetic to wear off as quickly as possible after surgery. TKX fills all of our requirements.
Although mixing Telazol® with ketamine and xylazine is not part of the manufacturer’s recommendation, there are many studies that substantiate its widespread use and safety. Board certified anesthesiologists advocate its use. Tens of thousands of cats have been safely anesthetized with TKX. Studies prove that it is reliable, predictable and safe. PDF Journal articles on TKX The onset of action and effects are predictable in our circumstances, and we are very comfortable knowing what adverse effects potentially occur and how to treat them.
There are unique characteristics of Telazol® that differ from more traditional anesthetics that users should know, although none of these characteristics is detrimental. Read the manufacturer’s insert for Telazol® for additional information. (wyeth.com/products)
2. Why do we use small animal xylazine?
Instead of using the large animal strength xylazine (100mg/ml), we use the small animal strength xylazine (20 mg/ml). Other clinics typically use the higher concentration because they need a longer period of anesthesia. The benefits of using a lower concentration are shortening the recovery time and reducing serious negative side effects, particularly vomiting and slow heart rate.
Vomiting at induction or under anesthesia is very uncommon at our clinic. The danger of vomiting is that the cat may choke on the vomit if it is too groggy to clear its airway. The cat can inhale or aspirate the vomitus into its lungs causing pneumonia or death. Because the flow of our clinic is efficient and speedy, the cats need a much shorter period of anesthesia than at many other clinics, including private practice, but particularly any spay/neuter clinics utilizing veterinary students for their surgeons.
3. Why do we add atropine to our cocktail?
To counteract the slow heart rate caused by xylazine, we include atropine in our TKX cocktail. The atropine blocks the xylazine mechanism that slows the heart rate. This maintains a higher heart rate during anesthesia, surgery and postoperatively. Another benefit is that atropine inhibits profuse salivation that can occur under sedation and prevents its interference with anesthesia via mask.
4. Why do we put the atropine in a separate sterile vial?
The atropine comes in a 100 ml vial. If we use draw every dose directly out of this vial, the repeated needle pokes through the rubber stopper cuts off tiny slices of rubber that fall into the vial. It is possible that a small piece of rubber stopper could be pulled up into the syringe and injected into a cat. By making smaller aliquots of atropine in smaller vials, we reduce the number of times a needle goes through the rubber stopper and eliminate the risk of rubber fragments in the atropine. We discard the 10 ml vial when it is emptied.
5. Why don’t we routinely use yohimbine?
Yohimbine reverses the anesthetic effects of the xylazine portion of our cocktail; it does not reverse all components of the anesthesia. Using yohimbine hastens the recovery time, but does not completely awaken the cats. We usually do not need to shorten anesthesia at our clinic. Most of our patients recover promptly after surgery, because we have administered low doses of injectable anesthetics and relied on gas anesthetic for the surgical plane of anesthesia.
We typically use yohimbine for any cat that we are especially worried about, such as late term pregnancies, cats that experienced respiratory arrest on induction, frail or sickly cats, cats that received unintentionally high doses and cats that experienced rapid or unexpectedly deep sedation from their first dose. If a cat is too sedated when discharge time approaches, then we consider using yohimbine. Basically, if we are worried about the status of a cat, then we use yohimbine to accelerate recovery.
STEP 1: BEFORE SEDATING THE CAT
From the Daily Anesthetic Log Sheet to cat selection and assessment, we increase efficiency and safety through simple protocols.
Read More
Before Sedation
Estimate Weight
Daily Anesthesia Log 1-35
Daily Anesthesia Log 36-70
Why We Do it This Way
1. Why do we try to get accurate weights instead of just guessing, or using “small, medium, large” doses like most TNR clinics?
Our primary reason to weigh or estimate weights is that we believe more accurate dosing of anesthesia increases the safety of anesthesia. Also, because we complete prep and surgery rather quickly, we need less total anesthesia time and smaller doses are appropriate. Lastly, by dosing more accurately, we use less anesthetic and save money.
STEP 2: THE INJECTION
Watch videos of our selection of techniques to restrain cats for injection. Our special techniques increase cat and human safety and save thousands of dollars per year. Reduce risk during those precarious minutes after injection of anesthetic.
Read More
Anesthetic Injection
Dose Chart
CPR
Why We Do it This Way
1. More information about the Dose Chart.
We began dosing cats using a simple 0.02 ml of TKX per pound. In the first year, we observed that we could lessen the dose for larger cats. Over time, dosing evolved to a sliding scale instead of a straight “per pound” dose. Also, our target is a lighter plane of anesthesia, because we add isoflurane when needed for a proper surgical plane of anesthesia. For programs that require 1-2 hours of anesthesia and do not have access to isoflurane, our chart may not be appropriate.
2. Why do we want to minimize the anesthetic dose?
We believe that unnecessarily deep anesthesia is the most common reason for cats to die unexpectedly. Anesthetics suppress heart and lung functions that are vital to survival and safe recovery.
Even young, healthy individuals can experience different responses to the similar doses. Thus, minimizing anesthetic doses reduces the occurrence of adverse effects and the risk associated with anesthetics, particularly in cats with unknown medical histories and conditions. Of the thousands of cats that come through our clinic, some are sure to have underlying illnesses that affect their responses to anesthetics.
Since we aim for a low dose of anesthetic, the magnitude of an accidentally high dose is mitigated, if we overestimate a cat’s weight. Lower anesthetic doses also hasten recovery, further reducing risk. Our mantra is simply that a light cat is better than a dead cat. We strive to minimize the dose of injectable anesthetic in every cat.
3. Why do we draw up the atropine into the TKX instead of mixing atropine into the TKX?
There are two reasons that we separate the TKX and atropine. First, if we have a cat that has received its first dose of anesthesia/atropine but needs a little more, then we can simply give more TKX without giving more atropine. Keeping the TKX separate allows us to administer only TKX when needed. Second, we are not aware of any information showing long-term compatibility or lack of compatibility between atropine mixed with TKX.
4. What happens if you accidentally draw up extra atropine?
If we accidentally overdraw the atropine by a small amount, then we remove the needle from the atropine bottle being careful not to push the extra atropine back into the bottle. Instead, we are careful not to mix the atropine and TKX. Because the atropine is in the needle, hub and closest to the syringe tip, we simply squirt out the excess amount to our desired dose before mixing the TKX with the atropine. If we overdraw by a large amount, we discard the entire dose and start over.
5. Why does the TKX and atropine need to be mixed in the syringe?
By drawing the atropine second, the needle, the syringe hub and the tip of the syringe are filled with atropine (approximately 0.07 mls) in addition to the intended dose that is in the syringe. If we inject the cat without mixing, then 0.07 mls of our injection would be pure atropine; this would displace a significant portion of the TKX. Mixing the contents improves the reliability of our dosing regimen. We used this technique successfully since 1997.
6. What action is needed if the anesthetic is accidentally given intravenously?
Intravenous injection of the anesthetic produces immediate sedation. With rapid induction, the cat may stop breathing. Intravenous sedation is typically immediate and profound, but it is not fatal as long as the cat is well monitored and respirations are maintained.
7. Why do we keep individual Medical Records instead of a running log sheet for each station in the clinic?
We prefer to keep detailed information on each cat on a single document so that we have all pertinent information at hand if a complication develops. Also, we may send home a copy of the Medical Record for the caretaker to see exactly what was done. If there is any complication after the clinic, the caretaker can show the Medical Record to a veterinarian, if such a visit is indicated.
8. What should be done if a cat starts to vomit under anesthesia?
If a cat vomits after receiving anesthetic or at any time while sedated, we immediately pick up the cat and hold its head lower than the rest of its body. Holding the head down encourages vomitus to drain out of the cat’s mouth. This position encourages material to fall out of the mouth instead of being inhaled or aspirated into the lungs. We never insert our fingers into the cat’s mouth, because they may bite down and cause serious injury. We may use a cotton tip applicator or spay hook to rake thick material (usually food) out of the cat’s mouth.
Vomiting is typically transient. After the initial episode ends, the cat usually does not vomit again. The vomiting incidence is low at our clinic, in part, at least, because we use a very low dose of xylazine.
Cost Saving Tips
1. Sharps disposal
Disposal of sharps (needles, scalpel blades) is charged per container. Filling the container with syringes, vaccine vials or other materials wastes space, which wastes money. Discarding the needle into the sharps container and discarding the cap in the garbage can also allows make more efficient use of the sharps disposal container.
2. Reusing syringes saves thousands of dollars each year
Reusing syringes saves thousands of dollars each year. For TKX and buprenorphine, we reuse the one syringe for each drug all day but we use new needles for each cat. We save money in two ways, primarily in the cost of anesthesia. By not discarding the 0.07 ml of anesthetic that remains in the syringe tip and needle hub after injection, we save thousands of dollars.
Although 0.07 ml does not sound like much, when multiplied times 8000 surgeries in one year, we save up to 560 mls, almost $4000 of anesthesia that would be otherwise discarded. There are special steps to be taken to maintain safety and maximize the recovery of anesthetic. See Procedures section for details on technique.
STEP 3: AFTER THE INJECTION
Specific steps after sedation prevent problems down the road and eliminate confusion.
Read More
Why We Do it This Way
1. Why do we use fleece instead of towels?
Fleece is superior at preserving the cat’s body temperature. Most cats lose body heat under anesthesia, so maintaining body temperature is imperative. Fleece also provides a good barrier against contamination, because fluids wick into the fabric instead of soaking through and contaminating surfaces below. The fabric is durable and does not deteriorate after bleaching with each wash. All of our fleece has been donated.
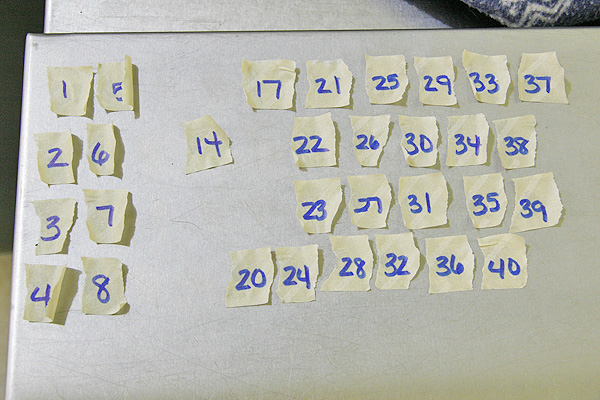
2. Why do we make masking tape labels before the clinic?
By having ID number labels made prior to sedating any cats, we have a quick visual method at any point in time to know which cats have been sedated and which cats remain. This is helpful if an individual needs their cats done earlier, or if we think we are finished but there is still one label unused. Having labels made in advance also provides a reminder for us to label the cat before moving into prep. Making labels in advance saves time during a busy clinic, simplifies the process and allows more focus on the cats.
3. Why don’t we use preprinted labels for the cats as we do for the carriers and Medical Records?
The masking tape sticks better to cat’s fur than preprinted labels. Proper identification is vital any time the cats are out of their carriers, thus, the ID number must adhere very well.
4. What is cryptorchid and how do we determine if a cat is cryptorchid?
5. When do we suspect pyometra?
6. Why don’t we express the male cats’ bladders?
Cost Saving Tips
1. Scales to weigh cats
No need to purchase expensive feline scales at $150. Digital scales for weighing babies work well for cats, are durable and easy to clean and cost about $40.
2. Product discounts for shelters
If you are a registered 501©3, many companies offer discounts on items commonly used by shelters. We particularly use shelter pricing on Idexx SNAP® feline leukemia tests and vaccines. Sales representatives of the individual manufacturers have information on which products may be available under a shelter program.

Surgery Prep
FIRST THINGS FIRST
The surgical prep station is the busiest, most multitasking station in the clinic. Multiple cats are present at once, each needing a multitude of services. Like a choreographed ballet, volunteers must know their roles and work well amidst a fast pace.
Read More
Before Starting Prep
Approach to CPR
Why We Do it This Way
1. What special handling do late term pregnant cats require?
We try to dose these cats with a very light dose of injectable anesthesia and then add isoflurane gas in order to hasten recovery after surgery. If the cat is known to be pregnant when admitted, then we try to do its surgery earliest in the day to allow more time for monitoring its recovery. Once the cat is sedated, then we keep her tilted her side until she has to be positioned for prep and surgery. We keep her tilted, because when she is on her back, the weight of the feti and uterus can compress the caudal vena cava, the large vein that supplies blood to the heart. This reduces blood flow returning to the heart and increases risks of anesthetic complications. By tilting the cat, the uterus slips off to the side and relieves pressure from the vena cava. When we prep her, we put her directly on her back. Then when prep is complete, we cover the prepped area with chlorhexidine soaked gauze and tilt her again, being careful to maintain the sterile field. Once she is in surgery and on oxygen, there is less risk, but we still monitor her breathing and mucous membrane color very carefully.
2. What are the typical effects observed with the type of anesthesia that we use?
Usually the cats’ eyes remain completely or partially open which gives the appearance of them being awake, however, the Telazol® works in a way that many body reflexes remain active unlike other anesthetic agents. Other anesthetics typically cause complete muscle relaxation. It is important to remember that whether a cat has reflexes is not an indicator of whether it can perceive pain! In other words, cats can be stiff and have some intermittent movement, yet still have no pain perception. While on Telazol, some cats have rigid and/or extended legs, while others are completely limp. Some cats may lift their heads while others are relaxed with both eyes closed. Telazol® affects cats differently from some of the other anesthetics. For a more complete description of its effects, please read the manufacturer’s drug insert. (wyeth.com/products)
3. What happens if a cat doesn’t appear to be breathing?
All volunteers are instructed to monitor cats for regular breathing. If there is any inkling of distress or lack of breathing, either the techs or volunteers notice it and immediately alert the lead tech or anesthesia tech. Without hesitation, we get out the cat and check the gums / tongue to see whether the cat is pink or blue. If it is pink, then we watch for a breath. Some cats breathe very slowly and infrequently and are actually ok. If the cat’s mouth is blue, then we start chest compressions while we feel for a pulse. Depending on what we find, we follow through our own algorithm for emergencies. Read more: CPR Document
4. What should be done if a cat starts to vomit under anesthesia?
If vomiting goes unnoticed, then the cat's risk inhaling food, bile, etc. If a cat vomits after receiving anesthesia or at any point during sedation, we immediately grab the cat and hold its head lower than the rest of its body. Holding the head down encourages vomitus to drain out of the cat’s mouth. This position allows anything vomited up to be expelled instead of inhaled. If the cat vomits food, we may use a cotton tip applicator or spay hook to clear out the cat’s mouth. We never insert our fingers into the cat’s mouth. They can bite down very hard and seriously injure someone. After vomiting, the cats are usually fine, and they do not vomit again. We have never had a cat aspirate, and our vomiting incidence is very low. This may be because xylazine is most likely to cause vomiting, and we use the lower concentration of xylazine in our anesthetic cocktail.
THE HEAD SIDE OF THE TABLE
Microchip scan, ear tip, penicillin injection, rabies vaccine, FVRCP vaccine, flea control. Keep it organized and do it well.
Read More
Head Side of the Prep Table
Ear Tip Template
Injection Site/Dose Chart
THE TAIL SIDE OF THE TABLE
FeLV test, gender, tattoo, surgical prep, fluids. Orchestrated with the other prep team, provide complete care with smooth flow.
Read More
WHY DON’T WE...?
Specific steps after sedation prevent problems down the road and eliminate confusion.
Read More
ABNORMAL FINDINGS
Out of thousands of cats that visit our clinic, abnormalities are imminent, however, not all require treatment. Read about a few common abnormalities and what to do about them.
Read More
Cost Saving Tips
1. Sharps disposal
Disposal of sharps (needles, scalpel blades) is charged per container. Filling the container with syringes, vaccine vials or other materials wastes space, which wastes money. Discarding the needle into the sharps container and discarding the cap in the garbage can also allows make more efficient use of the sharps disposal container.
2. Reusing syringes saves thousands of dollars each year
Reusing syringes saves thousands of dollars each year. For TKX and buprenorphine, we reuse the one syringe for each drug all day but we use new needles for each cat. We save money in two ways, primarily in the cost of anesthesia. By not discarding the 0.07 ml of anesthetic that remains in the syringe tip and needle hub after injection, we save thousands of dollars.
Although 0.07 ml does not sound like much, when multiplied times 8000 surgeries in one year, we save up to 560 mls, almost $4000 of anesthesia that would be otherwise discarded. There are special steps to be taken to maintain safety and maximize the recovery of anesthetic. See Procedures section for details on technique.
3. Donated fluids, needles, IV administration sets, insulin syringes
One supporter brings leftover IV fluids from the medical office where she works. The fluids are fresh, sterile and headed for disposal. Occasionally, supporters have leftover fluids, needles, insulin syringes and/or IV administration sets when their pet dies. We put these donated items to good use and owners are comforted knowing that something positive results from their loss.
Surgery Suite

The tranquil atmosphere of the surgery suite contrasts markedly with the fast-paced, multitasking prep table. Surgeons are sequestered in their 8’ X 10’ suite and quietly, calmly perform a single task: surgery. Every aspect of our set-up evolved from efforts to save money, save space and maximize efficiency, comfort and safety.
Read More
Surgery: Set-up and Supplies
Buprenorphine Dose Chart
Why We Do it This Way
1. Why do we use over-the-bed (OTB) tables instead of heated stainless steel surgery tables?
Cost was the original reason that we bought OTB tables. When comparing the cost of $99 per table to the several thousand-dollar price tag on surgery tables, there was really no comparison. After using the tables for a couple of years, the surgeons began commenting that they like them better than stainless steel tables. OTB tables are narrower, so the cat is closer to the surgeon. This makes the surgeons more comfortable doing many hours of surgery, because they do not have to lean over to be close to the cat. The OTB tables have adjustable height, and with the addition of a heating pad, they are more than sufficient for feline spay/neuter. Additionally, the OTB tables are on wheels and weigh very little. We can rearrange the room when we have multiple surgeons and we can easily remove the tables for cleaning. The small size of the OTB tables allows us to have a smaller surgery suite and thus, maximize our space to its greatest efficiency.
2. Why do we use desk lamps instead of surgical lights attached to the ceiling?
The lamps also began as an economical decision that evolved to be something that we liked better than the expensive equipment on the market. The low technical level of spay/neuter reduces the requirement for high intensity lamps. At $10 each, the comparison between these lamps and the official $1500 surgery lamps was drastic. Besides cost, one benefit of the attachable desk lamps is that they attach to the surgery table, not to the wall. So when we rearrange the tables, the lights follow. The layout of our room is not dictated by where the surgery lamps are attached to the ceiling, because the lamps are attached to the movable tables.
3. Why do we use heating pads?
We use heating pads set only on low to help maintain body heat during the spay surgeries. Most cats begin losing heat immediately after being sedated, because the body is not moving. Muscle movement is what generates body heat, while fat keeps the heat contained. So when a cat is sedated and begins cooling off, we try to combat heat loss by adding heat externally. Pregnant cats, particularly those in later stages or with many feti, lose even more body heat once the uterus is exposed through the surgical incision. More time in surgery and more time sedated means more heat loss. Having the heating pads under the cat during surgery adds heat back to their bodies.
4. Why do we keep the heating pads on the low setting?
The veterinary professional field knows well that heating pads can burn. As such, any setting other than low is potentially too hot. When an animal is sedated, it does not feel the burn and cannot move away. Furthermore, heating pad burns are not apparent until days after surgery. We strictly forbid the heating pad settings to be above the low setting in order to protect the cats from unintentional burns.
5. Why do we use towels to position the cat instead of V trays, aka, thoracic positioners?
The towels are pliable, washable and accommodate the heating pad underneath. If we used the heating pad on the V tray, then the edge would stick up and interfere with the surgeon. Some people recommend rice-filled socks for heat and positioning. We considered using these, but decided against them because they are not washable and they can be overheated and potentially burn the cat.
6. Why don’t we tie the cats to the surgery table?
Tying the legs stretches out the body and tightens up the cat. While it prevents the cat from moving as the surgeon manipulates the tissues, tying the cats also stretches all the ligaments inside, including all of the ligaments supporting the ovaries and uterus. When the ovarian and uterine ligaments are tight, surgery becomes more difficult to expose the ovaries and uterus. There simply is less slack in the ligament which means the surgeon must make a larger incision to expose the uterus and ovaries. Leaving the legs untied allows slack in the abdominal ligaments allowing easier and better surgical exposure through a smaller incision. A smaller incision requires less time and suture to close while reducing post-operative discomfort for the cats.
7. Why did we choose buprenorphine instead of other pain relief options?
The primary benefits of buprenorphine over other pain medications are safety and length of efficacy. Most people associate pain relievers with drowsiness, but buprenorphine has less sedative effect than both narcotic and opioid pain relievers. Cats do not have noticeably prolonged recoveries after receiving buprenorphine. Side effects of potent pain relievers, such as morphine, are primarily depression of the heart and lung function. Although buprenorphine is 30 times more potent pain a reliever than morphine, respiratory depression is a rare side effect.
Non-steroidal anti-inflammatory drugs (NSAIDs), such as Meloxicam®, are contraindicated during anesthetic events. NSAIDs can cause harm to the gastrointestinal tract and kidneys.
Butorphanol (known as Torbutrol® and Torbugesic®) only provides about 1-2 hours of pain relief in the cat. We consider this duration insufficient especially considering that we can provide 8-12 hours of additional pain relief by using buprenorphine. When used alone, the anesthetic cocktail of Telazol®, xylazine and ketamine provides significant pain relief. At an average cost of 50 cents per dose, we believe providing additional pain relief with buprenorphine is worth the expense and poses no additional risk to the cat.
8. Why don’t we give buprenorphine to every cat?
By itself, the anesthetic cocktail provides significant pain relief to the cat. Xylazine is a well-established pain medication for abdominal procedures and ketamine is recognized to offer effective pain relief to superficial tissues. When used alone, Telazol® provides mild to moderate levels of pain relief in cats. We believe that the combined action of these three drugs provides significant levels pain relief for extra-abdominal procedures.
9. Why do we only use a mask and not an endotracheal tube for anesthesia?
In general, endotracheal intubation uses more time under anesthesia and requires more expertise to install. Using tubes requires that someone individually monitor the cats at recovery so they do not wake up, chew the tube in half and inhale the lower end of the tube. Endotracheal tubes can be irritating to the trachea, especially when experiencing spasm of the larynx. Irritation can lead to coughing and sore throat after anesthesia. The benefits of intubation are the preservation of a patent airway and the direct administration of oxygen during prolonged procedures.
Masking cats is simpler, faster, cheaper and very safe. We have used isoflurane / oxygen via mask since 1998 and have been very happy with its performance. The GasVak system maintains fresh gas flow through the mask to eliminate exhaust gases and provide sufficient oxygen to the cat. Most of our cats are in surgery for less than ten minutes, not a prolonged period. One of the benefits of Telazol® is the preservation of many reflexes, such as the laryngeal reflex. This reflex complicates endotracheal intubation, because touching the larynx causes spasm. Forced placement against the spasm can irritate the larynx. Topical anesthesia can relieve the spasm, but we do not believe the effort to intubate is necessary. We believe the 30,000 surgeries performed under our protocol is proof of safety and efficacy.
10. Why do we do surgery on cats with upper respiratory infections?
Many cats that come to us have only one opportunity for spay/neuter. If the cat gets trapped and brought to our clinic, we do everything possible during this opportunity to help the cat. Most caretakers have no facility to hold cats for treatment prior to surgery. Many lack the time, money or skill to medicate a feral-behaving cat, if indicated for upper respiratory infection (URI). Since 1997, we have altered many cats with URIs and developed ways to maintain safety.
11. What complications do we see from URI and surgery?
A cat with severe nasal congestion relies on breathing through its mouth. When sedated, the cat cannot voluntarily or consciously open its mouth. When we put the cat’s face into an anesthetic mask, we force the mouth shut. If the cat cannot breathe through its nose and we have shut its mouth, then the cat can become hypoxic and suffocate.
12. How do we avoid complications from URI and anesthesia?
For cats with severe URI and nasal congestion, we may increase the dose of injectable anesthetic to avoid the need for gas anesthetic. Another option is to use a small mouth gag to hold open the cat’s mouth along with using the mask and isoflurane. We fashion a mouth gag by cutting a small segment of a 1 cc syringe and placing the open ends over an upper and lower canine tooth to hold open the jaws.
13. What happens to the tissues after the clinic?
In an effort to learn more about free-roaming cats, we are involved in several studies. If cats qualify, then their tissues may be preserved for further study. If not used for education, the tissues are bagged, frozen and picked up by a service that handles biological waste.
Cost Saving Tips
1. Surgery Tables: Using over-the-bed tables
Compare the price of $99 per over-the-bed table to the two thousand dollar or more prices of stainless steel surgery tables. The savings are huge. Now our surgeons prefer OTB tables, because they are narrower which positions the cat closer to the surgeon. This increases comfort during many hours of surgery, because the surgeons do not need to lean over to do surgery. The OTB tables have adjustable height, and with the addition of a heating pad, they are more than sufficient for feline spay/neuter. Additionally, the OTB tables are on wheels and weigh very little. We can rearrange the room when we have multiple surgeons, and we can easily remove the tables for cleaning. The small size of the OTB tables allows us to have a smaller surgery suite and thus, maximize our space to its greatest efficiency.
2. Heating pads, not heated tables
The $20 for a heating pad does not compare to the several thousand-dollar cost of a heated surgery table. For 5-15 minute spays, heating pads set on LOW are more than sufficient.
3. Surgery lamps
Desk lamps that attach to the surgical tables provide plenty of lighting for spay surgeries. Even the most complex of spays does not require intense lighting. Surgical lights start at $1500 each. We have used $20 desk lamps for ten years with happy surgeons.
4. Reusing syringes saves thousands of dollars each year
For buprenorphine, we reuse the one syringe for each drug all day but we use new needles for each cat. We save money in two ways, primarily in the cost of medication. By not discarding the 0.07 ml of anesthetic that remains in the syringe tip and needle hub after injection, we save thousands of dollars. Although 0.07 ml does not sound like much, when multiplied times 6000 spays in one year, we save up to 420 mls, almost $1500 of drug that would be otherwise discarded. There are special steps to be taken to maintain safety and maximize the recovery of anesthetic. See Procedures in above section for details on technique.
AT THE END OF SURGERY
Depending on the complexity of the surgery, cats may require additional procedures once the surgery is complete. Blood loss, dehydration, hypothermia and complications require additional attention.
Read More
Why We Do it This Way
1. Why do we use initials instead of recording the surgeon’s full name?
Using initials prevents most caretakers from knowing the full name of the surgeon. We have had incidents of caretakers locating a veterinarian that volunteered and then contacting them in their private practice for free veterinary advice. This scenario is clearly undesirable. We make a concerted effort to be grateful for the vet’s volunteer time for performing surgery and prevent additional obligations after the clinic.
2. Why do we record details about surgery?
Details regarding any non-routine surgery may be important after the clinic. In the uncommon event that a cat develops complications after discharge, we review the record for anything unusual noticed during surgery, such as abdominal fluid, prolonged bleeding, abnormal tissues, etc. Having more information may improve the treatment approach for a cat with problems after surgery.
3. Why do we use swaged on suture instead of cassettes and reusable needles?
Inch per inch, swaged on suture costs more than suture that is supplied on cassettes or reels. However, most surgeons are faster with swaged on suture, because it is simpler to handle. Reducing surgery time is best for the cat and translates into more surgeries per hour and less anesthetic for the cat. Additionally, the reusable needles needed for suture on a reel become dull after repeated use. Dull needles cause more tissue damage and inflammation.
4. Why do we reverse the anesthesia in some cats?
We reverse anesthesia to hasten anesthetic recovery. Although we have a very low complication rate, anesthesia is always a risk in any cat. Because anesthesia lowers blood pressure and heart/lung function, anesthesia can compound or exacerbate complications that develop during the anesthetic period, such as slow breathing, difficult breathing or respiratory arrest (no breathing). The first step to treat anesthetic complications is to stop administering more (remove isoflurane) and secondly, to reduce what has already been administered. This is accomplished by flushing isoflurane from the anesthetic lines, increasing oxygen flow to help remove isoflurane from the cat’s body and using yohimbine to remove the effects of the xylazine.
If a surgery is especially complicated, we may reverse part of the injectable anesthetic with yohimbine. We often reverse cats that are at risk for hypothermia (low body temperature) after surgery, such as those that are very thin and cats that are in the mid to late stages of pregnancy. When the uterus is exposed from the abdomen, the cat’s body loses heat into the air from the uterus. These cats can be very chilled after surgery, so we monitor them even more closely. We may also reverse cats done later in the day, if the caretakers need to pick up the cats. Cats that had any complication prior to surgery, including rapid, deep induction, respiratory arrest, or outward signs of illness, will also be reversed immediately after surgery.
Neuter
NEUTER SET-UP
Routine neuters are performed at the prep table. Licensed veterinarians typically perform the neuters; occasionally, veterinary student externs volunteer and perform neuters under the instruction of our licensed veterinarians. (Externs are not allowed to perform spays.) An assistant typically holds the legs for optimal position during the procedure.
Why We Do it This Way
1. Why do we perform neuters on the prep table instead of in the surgery suite?
Routine neuters are not considered invasive surgery, because the incision is only through the skin and not into the abdomen. The procedure only requires about one minute from start to finish and does not require a high degree of concentration on the part of the surgeon. The surgery suite is reserved for invasive surgeries. The room is sequestered to maintain a calm, quiet, atmosphere without distractions.
NEUTER SUPPLIES
Maintain high quality surgery while saving money.
Read More
Why We Do it This Way
1. Why do we reuse scalpel blades?
Any cut from a sharp blade bleeds more than a cut from a dull blade. This is a basic principle of tissue and surgery. A vessel being severed from trauma or a dull instrument experiences more microscopic damage to the vessel tissue. The damage is beneficial, because it stimulates contraction of the vessel walls and releases chemicals that activate clotting. Because the vessel constricts, blood loss is reduced and clotting is accelerated. New sharp, scalpel blades are preferable in typical surgery, because we are trying to minimize tissue trauma. In neuters, however, a little bit of tissue trauma benefits the cats by reducing bleeding and enhancing clotting. The reuse of the scalpel blades helps blunt the sharp edge from a new scalpel blade as the cut is made through the scrotal skin.
2. What do we do if a cat seems to be bleeding excessively from his scrotum after neutering?
When a cat has pronounced scrotal bleeding, the cat is almost always a gigantic tomcat. Bigger toms bleed more than smaller cats, because bigger toms have larger blood vessels, and their tissues are thicker. We expect some bleeding from all the neuters, because the standard surgical procedure does not involve suturing or tying all layers of tissue, including the skin incision. The normal amount of bleeding usually accumulates in the empty scrotum and forms a clot.
If the cat bumps around during recovery, he can dislodge the clot that formed in his scrotum. In this case, he will appear to have clotted and then start bleeding again. With time, he will form another clot.
If the cat is still fully sedated and bleeding significantly, then we may ask a volunteer to apply pressure and/or a cold pack to the scrotum to help encourage blood vessel constriction and clot formation. The ice should not be on the cat’s body, just on the scrotum, to avoid chilling the cat. Occasionally, the veterinarian applies a few drops of epinephrine to the bleeding tissues; epinephrine constricts blood vessels and helps stop bleeding. Sometimes the surgeon preempts the bleeding issue in large tomcats by ligating the tunics using the suture from a cassette, which is cheaper than the suture sold in individual packs.
3. If we use cold sterilization on the blade, why do we autoclave the neuter clamps?
The blade is very smooth and flat, thus, it is easy to wipe clean with gauze. Once submerged in the chlorhexidine, the blade is thoroughly disinfected. Infectious disease experts confirmed that there is virtually no chance of transmitting blood borne diseases with our protocol, because the organisms do not survive cold sterilization. While the same philosophy could apply to disinfecting the neuter clamps and ear clamps, these instruments are more difficult to clean due to the ridges along the jaws. If any blood residue were to remain on the clamp, then the disinfectant may not work well. The least expensive neuter clamps and ear clamps are sufficient for neuters and ear tipping, so purchasing one clamp per cat is not a significant expense.
Cost Saving Tips
1. Exam gloves for neuters
With the surgical technique for performing a cat neuter, most veterinarians do not wear sterile surgical gloves. New exam gloves are clean, sufficient for routine neuters and cost less than sterile surgical gloves. Exam gloves are the standard for neuters in most veterinary practices.
2. Neuter clamps: Human hospital surplus
Human hospitals dispose of decent stainless steel instruments every day. Many of those instruments are more than sufficient for their purposes of feline spay/neuter, such as tissue forceps and scissors. Surgical nurses are happy to collect these instruments for our use.
3. Emesis basins for cold sterilization
Human hospitals discard large numbers of basins each day. These work great for cold sterilization receptacles.
ADDITIONAL ANESTHETIC
Some cats require more either another dose of TKX or masking with isoflurane. We prefer isoflurane over adding an injection. Because we do not perform physical exams prior to sedation and cats come without medical histories, we balance minimizing their injectable anesthetic dose with humane and effective anesthesia.
Why We Do it This Way
1. Why do we prefer gas anesthetic to augment the injectable anesthetic when cats are too lightly sedated?
Because of the nature of the TKX cocktail, one component of it wears off sooner than the others. Thus, a cat could become light, yet still have a significant amount of parts of the anesthetic cocktail in its system. When we administer an additional amount of TKX, then we risk a high dose of the components that are slower to wear off. Since the neuters only require a minute or less of surgery, the isoflurane by mask is the perfect way to get them sleepy quickly and have them awaken rapidly afterward. Using the isoflurane as a boost for more sedation is not only safer, but also faster and less expensive.
CRYPTORCHID CATS
Many organizations consider cryptorchid surgeries as optional. There are pros and cons to doing them, and we provide some tips for those who operate them.
Read More


Additional Procedures
With a love for cats comes the desire to treat the problems of each and every one. But life sets limits on everything. We learned early on that in order to maximize spay/neuter, we could not fix every problem for every cat. We focus on spay/neuter, but we do not ignore cats with simple problems that have simple solutions. Learn the process that we developed to triage cases and make decisions about performing additional procedures.
Read More
Triage of Additional Surgical Procedures
Why We Do it This Way
1. Why do we perform any additional procedures when our mission is limited to spay/neuter?
We only consider additional procedures for the free-roaming cats. Any owned or pet cats are referred to local veterinarians. The free-roaming cats are cared for by the caretakers but not to the intimate degree of pet cats. They cannot simply be picked up and brought to any vet when there appears to be a problem. Many vets will not see cats that are not tractable, so even if a caretaker sought veterinary attention, they would be challenged to find a willing vet. For these reasons, it makes sense to try to accomplish all that we can for a free-roaming cat during one visit, one anesthetic period and one holding period with the caretaker. The problems we address are triaged to have predictably positive outcomes and not require ongoing or long-term care. We help as many cats as we can as much as we can as efficiently as we can.
2. Why do we only admit free-roaming cats for spay/neuter and not for other procedures?
Our mission clearly states that our work is limited to spay/neuter, and our donors expect their dollars to pay for spay/neuter. Some organizations spend hundreds and even thousands of dollars to save a single cat. Our focus is high volume, high quality spay/neuter which means spending small amounts of money to spay/neuter many, many cats. If we were to also provide standard medical care to cats that are already altered, then less money would be available to spend on spay/neuter.
Local veterinarians are notoriously worried that any non-profit spay/neuter programs will take away their clients, and thus, their revenue. We understand and respect their concerns. We have always maintained an excellent relationship and reputation with our local veterinary community, because we have kept our promise that we are only interested in spay/neuter. If we violate that promise, then we lose the support of the local veterinary community. Their support helps our organization in many ways and is worth protecting. Referring other procedures to local vets saves our money for spay/neuter and fosters the practices of local vets.
3. Why do we refer tame kittens/cats to local veterinarians?
Our donations are intended to pay for spay/neuter to end feline homelessness, so any “extra” procedures are limited to cats that we expect to never see a regular veterinarian. Pet cats can and will be taken to local vets, so we provide the spay/neuter and nothing else for them.
Local veterinarians are notoriously worried that any non-profit spay/neuter programs will take away their clients, and thus, their revenue. We understand and respect their concerns. We have always maintained an excellent relationship and reputation with our local veterinary community, because we have kept our promise that we are only interested in spay/neuter. If we violate that promise, then we lose the support of the local veterinary community. Their support helps our organization in many ways and is worth protecting. Referring other procedures to local vets saves our money for spay/neuter and fosters the practices of local vets.
COMMON PROCEDURES WE MAY PERFORM
When time and skills allow we declaw extra/imbedded toenails, perform enucleations, tail amputations, and simple hernia repairs in females, neuter extra-abdominal cryptorchids, flush and drain abscesses and extract abscessed or loose teeth.
Read More
Common Procedures We May Perform
Why We Do it This Way
1. Why do we declaw extra toes on feral cats?
We do not declaw all extra toes, in fact, we leave most of them alone. However, if we find a toe that grows from deep between other toes and risks getting an ingrown nail or already has an ingrown nail, then we will declaw that toe and nothing else. We have seen cats with a single extra toe that grows from deep between other toes and the nail has grown 360 degrees, full circle and is growing into the flesh. It is most common to see only a single problem toe per cat. However, we have seen a few cats with multiple problem toes and one cat with many ingrown toenails. Removing the claw permanently cures the problem. The extra claws are useless to the cat and are not used for fighting, climbing trees or catching prey. Extra toes are a birth defect and are unnecessary for quality of life.
2. Why would we consider releasing a cat to a free-roaming lifestyle with only one eye?
Enucleation is an improvement rather than a handicap. Think about the logic behind this issue. The eye being removed had no vision before the cat came to our clinic. If the cat appears healthy in other respects, then clearly it has adapted to being one-eyed just like so many pet cats that lose an eye. Since we remove pain and infection by treating the ruptured eye, then the cat’s quality of life is improved after enucleation. Survival and quality of life do not depend on having two visual eyes. We know of numerous one-eyed free-roaming cats that live normal lives. Keep in mind that we only consider this procedure, if the cat has met the other criteria that we have described.
3. Under what conditions would we not amputate the tail?
When a tail injury is very high on the tail, near where the tail attaches to the body, then we are concerned about spinal cord damage. Even though the important parts of the spinal cord do not enter the tail, the spinal cord can be damaged above where the injury occurred, particularly if the tail were pulled during the trauma. In order for us to proceed with a high tail amputation, we need to know that the cat can urinate and defecate normally to know that there is no spinal cord damage. We also need to physically have enough undamaged tissue available for a successful result. The veterinarian makes the assessment and decides whether a cat is a candidate for tail amputation or not. Keep in mind that we only consider tail amputation, if the cat has met the other criteria that we have described.
4. What is the typical course of action for an abscess in cats that go untreated?
How Mother Nature deals with abscesses is actually very interesting. Let us start with how they form. Cats have a disagreement and one bites another. The sharp tooth of one cat punctures the skin of another. Unlike dogs, cats bite, puncture and pull away; dogs bite, hold and shake, which results in lacerations and tears in the skin. Because cats heal very well, the skin quickly closes over the puncture, leaving a deposit of bacteria in the warm, protein-rich environment of the cat’s body.
Most of the time, the cat’s immune system attacks the bacteria, kills them and all is well. In some circumstances, the bacteria get a head start and form an abscess, a pocket of pus. As the bacteria continue to reproduce, the pocket grows larger and pushes out on the skin. As pressure increases, the blood supply in the skin collapses. Without blood supply, a tiny spot in the skin dies, weakens and ruptures. When it ruptures, the pus leaks out. With drainage established, the cat can fight off the infection. When we find an abscess, we help this process by increasing or initiating the drainage and augmenting the cat’s fight against the bacteria with antibiotics.
5. Why doesn’t tooth extraction harm the cat’s chances of survival?
Infected teeth can cause pain and cannot become normal, healthy teeth again. They act similar to a splinter that is stuck in our skin: the body creates inflammation to try to get rid of it, and the inflammation will not go away until the splinter is removed. An infected tooth behaves similarly. The body tries to get rid of the infection and creates a lot of inflammation. Once the tooth is gone, then the infection and inflammation resolves. If the cat does not visit a veterinarian, eventually the tooth falls out and it heals. We can accelerate the healing process by removing the tooth while the cat visits us for spay/neuter. The teeth are not useful to the cat as they are, not needed for survival or eating. And we have seen many a cat with missing teeth that is in good body condition. Keep in mind that we only consider tooth extraction, if the cat has met the other criteria that we have described.
GENERAL
If any treatment involves suturing, we use only absorbable suture and/or surgical glue. We never use suture material that requires future removal.
Post Op


Although the Post Op station has few tasks, this station is no less important than the others. Cats require very close monitoring to avoid unforeseen complications. We designed a clear set of steps for returning cats after surgery, assessing their status and identifying and treating common post-operative complications. Be prepared for the unexpected.
Read More
Why We Do it This Way
1. Why do we use chlorhexidine instead of bleach to clean the carriers and traps?
Dilute chlorhexidine (CHX) solution is a good disinfectant and cleaner. It has very little fragrance, so there is no significant residual odor to bother people or the cats. The disinfecting action becomes denatured by any organic materials (urine, feces, saliva, food), however, we mainly use CHX solution for cursory cleaning, not for sterilizing the carriers and traps.
We do not use bleach for cleaning carriers, and many people ask why. Using bleach on the cat’s own carrier is unnecessary. If a cat comes out of a carrier and goes back into the same carrier, then the cat is not being exposed to anything foreign. We simply do not need to sterilize the carrier. People are not placed in sterile beds after surgery, so cats do not need sterile bedding after surgery either. Aside from lack of need, bleach is irritating to the skin. If cats come in contact with bleach, they can receive chemical burns, such as cracked paw pads. Bleach can also damage the carriers and traps, if not rinsed off. Additionally, bleach pollutes the indoor air in enclosed spaces/ rooms. Fumes in the air can be very irritating to cats and people.
2. Why do we return carriers to their original order instead of moving cats to a recovery area after surgery?
We prefer to keep the cats in the same room with us all day, so that there are always multiple sets of eyes watching them. Because we return cats to their original order, we know approximately which cats were sedated earliest in the day and therefore, which should be recovering first. For example, if we notice a cat at the beginning of the order that is not awake, yet many cats later in the order are fully awake, then we know quickly that there could be a recovery problem to consider.
3. Why do we prohibit more than one cat/kitten per carrier/trap for recovery?
Safety is the issue. Some cats recover smoothly and have no problem being with another cat, however, some cats awaken and hiss, bite and/or attack any other cat that is in the carrier. This is true even if the cats know each other and arrived together. Anesthesia alters the cat’s perception. Once they start to fight, the cats can be seriously hurt. Another serious concern is that a cat beginning to awaken may lie on top of another cat that is still heavily sedated. This can suffocate and kill the cat underneath. Another organization’s veterinarian warned us of this problem after such an incident occurred at their clinic.
4. Why do we place the cat in tail first?
We want to be able to see the cat’s face while we monitor its recovery. We need to know that the cat can breathe without any hindrance, such as the blanket over its face or its neck bent. When we reach in to assess the cat’s recovery, we can easily check jaw tone, the blink reflex, gum color and monitor the ear tip as needed.
5. Why do we place the tipped ear up?
When the ear tip is up, the incision is above the level of the heart. Keeping the incision elevated relative to the heart slows bleeding and encourages clotting.
6. Why do we put the cat in its carrier/trap without taking its body temperature?
The vast majority of cats recover well without heat supplementation. For years, we took post-operative body temperatures. We discovered that many times, the temperature had no correlation with how well the cat was recovering. For instance, a cat could appear wide awake, yet have a low temperature. Volunteers would try warming an awake cat merely because the thermometer indicated that the cat was cold. Lots of time and energy went into monitoring the temperature and fewer people paid close attention to the cat's’ vital signs. All in all, we felt that the thermometer distracted more than it contributed to a safe recovery. Therefore, we use the thermometer sparingly. We prefer to rely on pulse quality and other vital signs for assessing the cats.
7. Why do we put cats in their carriers instead of on heating pads while they are waking up?
Most cats recover well without heat supplementation. Supplementing heat to cats that are already warm but are still sedated risks overheating the cats. We do not routinely take post-op body temperatures (see previous question) but will take the temperatures of cats that are slow to recover. We supplement heat on an individual basis for cats with low body temperature discovered during assessment for slow recovery. Some cats do not get cold during surgery, and if all cats were put on heating pads after surgery, some cats would become too hot.
8. Why do we reverse the anesthesia in some cats?
We reverse anesthesia to hasten anesthetic recovery. Although we have a very low complication rate, anesthesia is always a risk in any cat. Because anesthesia lowers blood pressure and heart/lung function, anesthesia can compound or exacerbate complications that develop during the anesthetic period, such as slow breathing, difficult breathing or respiratory arrest (no breathing). The first step to treat anesthetic complications is to stop administering more (remove isoflurane) and secondly, to reduce what has already been administered. This is accomplished by flushing isoflurane from the anesthetic lines, increasing oxygen flow to help remove isoflurane from the cat’s body and using yohimbine to remove the effects of the xylazine.
If a surgery is especially complicated, we may reverse part of the injectable anesthetic with yohimbine. We often reverse cats that are at risk for hypothermia (low body temperature) after surgery, such as those that are very thin and cats that are in the mid to late stages of pregnancy. When the uterus is exposed from the abdomen, the cat’s body loses heat into the air from the uterus. These cats can be very chilled after surgery, so we monitor them even more closely. We may also reverse cats done later in the day, if the caretakers need to pick up the cats. Cats that had any complication prior to surgery, including rapid, deep induction, respiratory arrest, or outward signs of illness, will also be reversed immediately after surgery.
WHAT TO EXPECT IN POST OP
Depending on the dose of anesthesia, time in prep and surgery, individual health, body temperature and other factors, the cats are at various stages of recovery when they leave surgery. Knowing what to expect increases safety for the cats, because the unexpected is more easily recognized. Also, volunteers are reassured by learning that what may appear disturbing is actually within the realm of normal. (See videos showing normal recovery behavior and assessment.)
Read More
Why We Do it This Way
1. How do we supplement heat to cold cats?
Sometimes we microwave the ice packs that accompany our vaccine shipments. These hold heat very well but are not durable for long-term use, so we slip them inside a plastic bag before using them. Hot packs can burn skin! They should feel warm to our touch but not be uncomfortable on our own skin. Once warm, we wrap the hot packs in a towel and place the packs alongside the cat’s torso. We place many layers of bedding on top of and underneath the cat to contain the heat. Heat is lost through the carrier bottom, if there is not sufficient insulation between the cat and the carrier.
PROLONGED RECOVERY: ASSESS & TREAT
Anyone who has worked in the veterinary medical field for long enough has experienced the sickening feeling of finding an animal dead in a cage. Sadly, it happens, because complications arise silently in recovery. Knowing how to assess cats during recovery is paramount and reduces unexpected complications. Recognizing problems as they arise allows time for treatment and avoids perpetuation into serious complications. Be sure you are doing everything you can.
Read More
Prolonged Recovery: Assess & Treat (Doc missing)
Why We Do it This Way
1. What are the basic ways to assess a cat’s recovery?
For people not trained in veterinary medicine, there are still ways to assess how well a cat is recovering. We consider a group of observations. Body position stages from most sedate to fully recovered: Unable to rise from its side (lateral recumbency); in lateral recumbency with legs moving; sternal; sitting or moving around uncoordinated; walking and coordinated.
- Blink reflex (do the eyelids blink when touched lightly?): Absent; barely present; moderately present; normal.
- Jaw tone (how much resistance felt when opening the cat’s mouth): None, very little; mild, a little tension but still fairly easy; moderate, requires more effort; normal, cat has full control of mouth.
- Muscle tone (how much resistance felt when flexing the cat’s legs): None, completely limp; mild resistance, a little tension but still fairly easy: moderate, requires more effort, legs are stiff; normal, cat has full control of legs.
Staff and volunteers trained to assess respiratory rate and quality, as well as pulse rate and quality use those parameters as well. These are most important when the cat is in the deepest stages of sedation. If the cat is clearly awakening well, then we do not need a more comprehensive assessment. If a cat is still deeply sedated, then we apply stimuli to aid in further assessment and to help arouse the cat from anesthesia. See below.
2. What type of stimuli do we use to assess and arouse the cat?
We apply the stimuli and reassess the cat’s level of recovery. In order of mildest stimulation to most aggressive.
- Rub the cat, pet very hard, speak loudly to it.
- Flip cat over to opposite side.
- Flex and extend legs vigorously.
- Pinch toes or toe webs
For a cat is that deeply sedated, applying the stimuli frequently and vigorously helps arouse them from sedation and encourage recovery.
3. How do we supplement heat to cold cats?
We apply the stimuli and reassess the cat’s level of recovery. In order of mildest stimulation to most aggressive.
- Rub the cat, pet very hard, speak loudly to it.
- Flip cat over to opposite side.
- Flex and extend legs vigorously.
- Pinch toes or toe webs
For a cat is that deeply sedated, applying the stimuli frequently and vigorously helps arouse them from sedation and encourage recovery.
MEDICAL RECORDS
The Medical Records are copied after the cats are awake. We review the records to insure that all the information is complete and accurate. Each Medical Record is copied onto a page with post-operative instructions on the back that goes home with the cat.
Except when we are making copies, the Medical Record is with the cat. With this system, we can immediately access the Medical Record, if there are any questions. We write the ID number on the copy, fold it in half and tape it to the front of the carrier. This provides a simple way to locate the cats when caretakers arrive for pick up. The original Medical Records are filed at the clinic.
Read More



Check Out
Although the Post Op station has few tasks, this station is no less important than the others. Cats require very close monitoring to avoid unforeseen complications. We designed a clear set of steps for returning cats after surgery, assessing their status and identifying and treating common postoperative complications. Be prepared for the unexpected.
Read More
Why We Do it This Way
1. Why doesn’t the veterinarian talk directly with caretakers at discharge?
Our veterinarian has a very clear job: to perform high quality, high volume spay and neuter surgeries. After a full day of surgery, the vet is ready and entitled to be “done”. We do not ask her to face the caretakers and myriad questions when the information sought is available from their regular veterinarian. Cursory information can be passed from our veterinarian to our technician and to the caretakers. Anything that is more involved needs to be pursued with the caretakers’ regular veterinarian.
2. Why do we refer people to regular veterinarians instead of treating free-roaming cats for all of their problems at our clinic?
Besides protecting the limits of our surgeon, we also protect the relationships of local veterinarians. We must preserve their position with their clients in order for us to maintain a positive professional relationship in the veterinary community. We have established ourselves in the veterinary community as providing high quality, high volume spay/neuter but nothing else. The veterinarians have slowly embraced us and supported our efforts. To violate that position by offering medical services, other surgical services, vaccines, advice and other treatments, we would put our community relationship at risk. We believe it is in the cats’ best interests for our organization to keep a narrow position in the community and maintain a positive position with local veterinarians. Furthermore, our donors expect their money to be spent on spay/neuter. Spay/neuter is our single mission and our funds are always directed into maximizing our surgeries. If we were to spend donated dollars on treatments other than spay/neuter, then we would be violating our mission and the promise that we make to our donors to fight homelessness through spay/neuter.
3. How warm is “very warm” for recovery?
A cat’s normal body temperature is about 100 degrees. Even if a room is 70 degrees and feels warm to us, the room is still 30 degrees colder than the cat! Body heat is created through muscle movement. Heat is retained in the body by insulation in the form of fat. So a thin cat that is too sleepy to move around will not be making body heat and will not have the body fat to retain the heat that is does have. Simply, the cat cannot keep itself from getting colder. As the cat gets colder, it cannot get rid of its anesthetic, thus, it can become more deeply sedated. As it gets more deeply sedated, it cannot move, cannot make heat and it gets colder. It is a vicious spiral that goes downhill. We estimate that “very warm” is about 85 degrees. We needed a number to give to people, because they do not always comprehend the importance of warm air being around the cats. Could we have selected another temperature? Of course. But 85 degrees is our reference.
4. Why do we have different feeding recommendations for different cats instead of a full meal as soon as possible for all cats?
Maintaining a normal blood glucose (sugar) is an important factor for recovering from anesthesia and surgery. Kittens and cats that are thin have smaller fat reserves and less energy stored in the liver. Thus, they may have difficulty keeping their blood glucose in the normal range. These kittens and cats are also at risk for low body temperature, so besides having less energy available, they may also require more energy to try to maintain their own body temperature. Shivering is nature’s way to create body heat, but it uses lots of energy. For these two main reasons, we try to avoid a kitten or cat experiencing low blood sugar by getting food into them as early as it is safe to feed them
There are risks with feeding any animal soon after surgery. Anesthesia slows down and sometimes stops the intestine from moving, so eating before the intestines can move might cause colic (stomach ache) or vomiting. To make matters worse, if a cat vomits that is still a bit drowsy, then it can inhale or aspirate its vomit. This can cause serious respiratory problems and death. Adult cats that have no risk of low blood sugar should not be fed until they are fully awake in order to avoid the complications that might be seen from feeding soon after surgery.
5. What factors do we consider when advising a caretaker when to release a cat?
In the perfect world, all cats would have homes. In the almost perfect world, all homeless cats would have a week in a warm, safe location to recover from surgery. In the real world, we strive for the best and take what we can get.
The most important consideration for releasing a cat is that the anesthesia has completely worn off, so that the cat is coordinated, can find its territory, food and shelter and can protect itself, if needed.
Human factors present many of the obstacles for holding cats. Most people do not have the facilities to house free-roaming cats in traps or carriers for more than a day or two after surgery. If we were to require that cats be held for a week after surgery, many people would not trap at all and the cats would be left free-roaming, unaltered.
In private practice, pet cats are sent home the day after surgery. Most are free to run around, go outside, climb, jump and be a cat. For the free-roaming cats, releasing the day after surgery is pretty realistic. The insecurity of doing this seems to emanate from the concern of, what if there is a complication? If a pet cat has a complication, then it is likely in a household that will notice the problem and seek out veterinary care, if needed. If a free-roaming cat is released and has a complication, then the caretaker may not notice it, especially if the cat does not return to eat for a day or two. The most likely complications are low appetite and low energy; these usually resolve on their own. Serious complications are rarely seen.
If inclement weather is expected, then it makes sense to hold cats until the worst is past. Our climate is fairly mild compared to other regions of the country. We get little or no snow in the winter. We do not experience hard freezing weather. If cats shelter from the wind and wetness, whether it is their own or manmade, then they survive through the weather as do the local squirrels, raccoons and other urban wildlife.
Our surgeon is very talented and knowledgeable. The spay incisions are typically no longer than 1 to 2 centimeters. Surgery time is typically under 7-8 minutes. Recovery from surgery is simpler and less complicated with high quality surgery.
6. Which cats are most at risk after discharge?
Cats that are less awake after surgery are at higher risk for problems than cats that are more fully awake. Especially if sleepy cats are not kept warm, then their ability to wake up from anesthesia is impaired. Any cats that have difficulty staying warm are at higher risk, as well. This includes kittens, thin adults and cats that became cold during surgery, namely, later term pregnant cats. Cats that were not in great condition prior to surgery are cats that we worry about more than robust, thriving cats.